A Dark Case of Cough
Gbonjubola Onawunmi MD1, Fellow; Evgeniya Angelova MD PhD2, Fellow;
Shawn P.E Nishi MD1 Associate Professor & Fellowship Program Director
1Division of Pulmonary, Critical Care & Sleep Medicine
2Department of Pathology, Division of Cytopathology
University of Texas Medical Branch
Case
An 86 year-old U.S army veteran presents with shortness of breath and chronic cough of several years duration. His cough is productive of white-yellow sputum without hemoptysis. Patient denies weight loss, fever, chills or night sweats. He is a former tobacco user (20 pack-years, quit 1976) and has moderate COPD (GOLD Class A, FEV1 1.50L, FVC 2.82L, FEV1/FVC 53). Past medical history also includes gastroesophageal reflux and diastolic dysfunction. In addition to being an army veteran, he also worked in the coal mines for 30 years. Physical exam is only notable for mild scattered expiratory wheeze bilaterally. He underwent a chest CT (Figure 1) as follow up for an abnormal chest x-ray. Based on the imaging findings, he then underwent flexible bronchoscopy (Figure 2) with endobronchial biopsies (Figure 3).
Figure 1a & Figure 1b
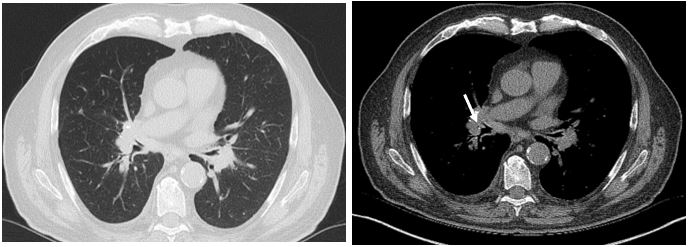
Figure 2
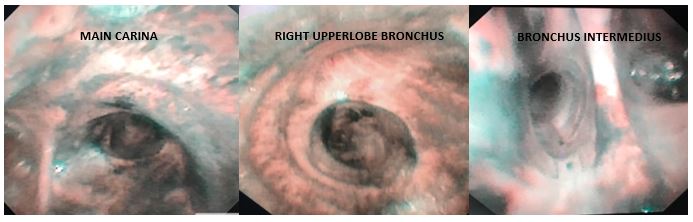
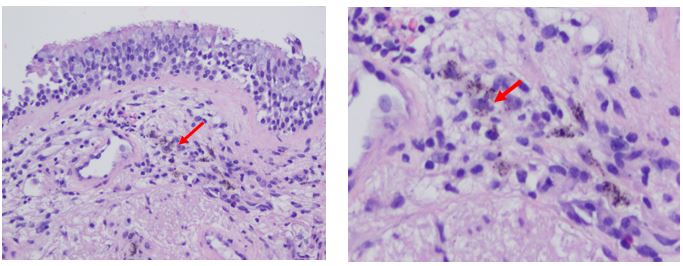
Figure 3
Question
What is the diagnosis?
- Tracheobronchial melanosis
- Endobronchial melanoma
- Bronchial anthracofibrosis
- Kaposi’s sarcoma
- Soot inhalation
C. Bronchial anthracofibrosis
Figure 1a CT thorax lung window: multiple innumerable punctate sub-centimeter nodules, narrowing of the right upper lobe bronchus and hilar adenopathy.
Figure 1b CT thorax mediastinal window: presence of right hilar calcification (white arrow).
Figure 2 Bronchoscopy: extensive mucosal anthracotic pigmentation of the carina, right upper lobe bronchus and bronchus intermedius depicted. Limited visualization of the distal subsegmental airways due to narrowing and extrinsic compression.
Figure 3 Pathology: fragments of benign mucosa with aggregation of pigment laden macrophages (red arrow) in the submucosa.
Discussion
This patient was diagnosed with bronchial anthracofibrosis from chronic occupational dust exposure from coal mining for >30 years. Anthracosis is the deposition of carbon containing particles in the airway mucosa and lung parenchyma, usually as a result of chronic inhalation of carbonaceous air pollutants or cigarette smoke1. Characteristic appearance on bronchoscopy is that of single or multiple black pigmented lesions within the central airway mucosa up to the secondary carina without airway distortion or fibrosis1,2.
Bronchial anthracofibrosis (BAF) is an extension of anthracosis and is characterized by the presence of dark pigmented bronchial airways, which may be narrowed or obliterated due to fibrosis1,3. Worldwide, BAF most commonly affects elderly women (age >60) from rural households in low-income countries with chronic biomass fuel exposure, particularly from cooking and heating in enclosed spaces3,4. Inhalation of smoke or coal causes deposition of carbonaceous particles in the airway mucosa, resulting in grey-black discoloration or “tattooing” of the airways. The mucosa at the branching points of the bronchi are most commonly affected, especially the right middle lobe and the upper lobe bronchi1,3. BAF has also been associated with active tuberculosis and certain malignancies5.
Symptoms include dyspnea, chronic cough, chest pain and hemoptysis3,5. Pulmonary function testing reveals an obstructive pattern +/- reversibility in the large majority of symptomatic patients5. Radiographic features include bronchial airway narrowing, fibrosis and architectural distortion, nodules, atelectasis particularly of the right middle lobe and mass-like lesions1,3,4,5. Hilar and mediastinal lymphadenopathy +/- calcifications may also be present5.
Biopsy demonstrates pigment-laden macrophages in the bronchial wall, submucosal hypertrophy and fibrosis with intact appearing epithelial lining4.
There is no established treatment regimen for patients with BAF. Symptom management includes inhalers commonly used in COPD, treatment of exacerbations with antibiotics and corticosteroids, management of associated conditions such as tuberculosis and avoidance of continued exposure1,4,5. In some cases, mechanical dilation +/- placement of endobronchial stents have been performed for stenotic areas5.
Incorrect Choices
Choice A. Tracheobronchial melanosis (TBM). Rare congenital pigmentation of the airways without associated fibrosis or symptomatology. Found incidentally on bronchoscopy performed for other reasons. A diagnosis of exclusion in the absence of occupational, environmental, infective causes and tobacco use history2.
Choice B. Endobronchial Melanoma. Usually as a result of metastatic malignant melanoma as primary lung melanoma is exceptionally rare. Patients usually carry a diagnosis of melanoma, in the instance that this is the first presentation, a detailed history and skin examination is warranted to identify the primary lesion. May present with cough, hemoptysis, recurrent pneumonias and atelectasis depending on its location2.
Choice D. Kaposi’s Sarcoma. Discrete pigmented lesions that can be found in the airway of patients with HIV/AIDS with low CD4 counts. Often in patients with existing cutaneous involvement. Can present with cough, hemoptysis and depending on location endobronchial obstruction and recurrent pneumonias6.
Choice E. Soot inhalation. Typically in the setting of burns and inhalational lung injury due to residential fires. In addition to black pigmentation of the airways there is also associated airway erythema, edema progressing in severity to airway ulceration and necrosis based on extent of exposure and flame characteristics2.
Other causes of pigmented airways on bronchoscopy include healed endobronchial tuberculosis scar, infections – particularly fungal (e.g. Aspergillus niger) and iatrogenic causes (e.g. chronic amiodarone use, chronic silver ingestion/inhalation)2.
References
-
Devarajan SR, Zarrin-Khamen N, Alapat P. Black Lungs and Big Nodes: A case of airway anthracosis with bronchial anthracofibrosis. Respiratory Medicine Case Reports 2018; 25: 9-11.
-
Gupta A, Shah A. Bronchial anthracofibrosis: an emerging pulmonary disease due to biomass fuel exposure. International Journal of Tuberculosis and Lung Disease 2011; 15(5): 602-12.
-
Jamaati H, Sharifi A, Mirenayat MS, et al. What do we know about anthracofibrosis? A literature review. Tanaffos Journal 2017; 16(3): 175-89.
-
Mirsadraee M. Anthracosis of the Lungs: Etiology, Clinical Manifestations and Diagnosis: A Review. Tanaffos Journal 2014; 13(4): 1-13.
-
Tunsupon P, Panchabhai TS, Khemasuwan D, et. al. Black Bronchoscopy. Chest 2013; 144(5): 1696-1706.
-
Valentin R, Drew P, Benninger L, et. al. Endobronchial Kaposi Sarcoma. Journal of Bronchology and Interventional Pulmonology 2019; 26(1): 62-5.


