A Relentless Cough: Late presentation of a developmental abnormality
Terace Thomas, Melissa Holtzlander
Case
A 2-year-old female born full term from a twin gestation presents for evaluation of persistent cough following pneumonia at 1 year of age. The cough is described as harsh, croupy, and present during the day and at night. The cough does not improve with Albuterol but does improve slightly with oral steroids, returning to baseline once these are stopped. She has no nasal symptoms, no exposures, and does not choke while swallowing, though sometimes parents feel that food gets caught when she swallows. Diagnosis was suggested on CXR that was obtained, as shown below.
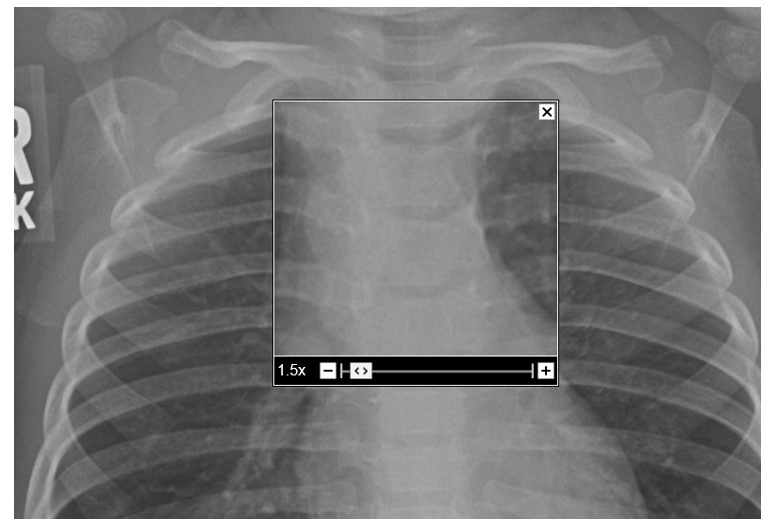
Figure 1. Chest x-ray
Question
What is the diagnosis?
- Airway malacia
- Laryngeal Cleft
- Congenital Lung Malformation
- Asthma
- Vascular Ring
Answer E. Vascular Ring
Discussion
Congenital vascular rings result from abnormal development of the aortic arch and its associated vessels during embryonic growth. Vascular rings (VR) make up 1% of total congenital abnormalities of the heart and vascular system. They can partially or completely encircle the trachea and esophagus resulting in airway or GI manifestations. These anomalies typically involve the aortic arch, the brachiocephalic arteries, and the ductus arteriosus. VR can take several forms, including double aortic arch (DAA), right aortic arch with left ligamentum arteriosum, innominate artery compression, and pulmonary artery sling. DAA is the most common form of vascular ring malformations. It is a complete VR and occurs due to failure of regression of one of the bilateral aortic arches during development. There are multiple types of DAA including: dominant right arch with small left arch, dominant left arch with small right arch, and balanced aortic arches.
Symptoms and presentations associated with double aortic arch vary based on the size of the ring formed by the vascular structures. Small restrictive rings can present early with respiratory failure after birth, apneic episodes, and cyanosis. Later presentations may include noisy breathing, persistent cough, recurrent lower respiratory tract infections, persistent dysphagia, failure to thrive, and exercise intolerance.
Diagnosing vascular rings typically involves a combination of imaging modalities, including:
- Echocardiogram – can delineate the type of double aortic arch
- Chest x-ray – may show the loss of the aortic knob and the indentation of the trachea.
- Barium swallow study – shows an indentation of the esophagus. The persistence of a bilateral indentation of esophagus on the frontal view is suggestive of a double aortic arch.
- CT (with IV contrast) or MRI – helps to elucidate the anatomy
- Bronchoscopy – can be used to evaluate the airway anatomy, observe the extent of compression or collapse, and rule out other anomalies
The treatment for vascular rings depends on the severity of symptoms and the anatomy present. Conservative management includes nutritional support and monitoring of respiratory symptoms. In symptomatic cases with significant airway or esophageal compression, surgical intervention is often required. Surgical procedures aim to divide or reposition the abnormal vascular structures to relieve the compression on the trachea and esophagus, thus improving respiratory and feeding functions.
The choice of surgical approach depends on the specific type and anatomy of the vascular ring. The most common surgical approach involves dividing and separating the abnormal vascular structure causing the compression. For example, in a double aortic arch, one of the arches may be divided so the trachea and esophagus regain their normal position.
The long-term prognosis for children who undergo surgical correction of vascular rings is generally excellent. Once the compression is relieved, most children experience significant improvement in their respiratory and feeding symptoms. They can lead normal, healthy lives without ongoing issues related to the vascular ring. Postoperative complications after surgery are infrequent but can include feeding intolerance, persistent coughing, stridor and wheezing. Phrenic nerve or recurrent laryngeal nerve injuries during surgery can result in diaphragm or vocal cord paralysis. The formation of an aorto-esophageal fistula can also occur. Other complications include persistent noisy breathing from tracheomalacia and/or bronchomalacia due to the presence of the vascular ring during fetal development.
It is important to note that the prognosis varies depending on several factors, including the type and complexity of the vascular ring, the age at which surgery is performed, and any associated congenital heart defects or other medical conditions. Close follow-up with pediatric specialists is typically recommended to monitor the child's progress and address any potential long-term issues.
References
-
Hanneman K, Newman B, Chan F. Congenital Variants and Anomalies of the Aortic Arch. Radiographics. 2017; 37:32-51.
-
Kau T, Sinzig M, Gasser J, Lesnik G, Rabitsch E, Celedin S, Eicher W, Illiasch H, Hausegger KA. Aortic development and anomalies. Semin Intervent Radiol. 2007; 24:141-152.
-
Licari A, Manca E, Rispoli GA, Mannarino S, Pelizzo G, Marseglia GL. Congenital Vascular Rings: A Clinical Challenge for the Pediatrician. Pediatric Pulmonology. 2015; 50:511-524.
-
Priya S, Thomas R, Nagpal P, Sharma A, Steigner M. Congenital anomalies of the aortic arch. Cardiovasc Diagn Ther. 2018; 8:S26-S44.


