Cystic lung disease
Van Holden, M.D.
Pulmonary and Critical Care Medicine Fellow
University of Maryland Medical Center, Baltimore, MD
Case:
A 33 year-old woman with a history of uterine fibroids and iron deficiency anemia presented with progressively worsening dyspnea on exertion for 2 years. She reported shortness of breath with climbing one flight of stairs. She had an associated dry cough and intermittent sharp right-sided chest pain.
Social History: Smokes 3-5 cigarettes per day for 15 years. Drinks alcohol occasionally. Prior history of smoking marijuana. Has had 1 sexual partner.
Vital signs and cardiopulmonary exam were normal. Basic labs and EKG were also normal. Due to an elevated D-dimer of 570 ng/mL, she had a CTA chest done.
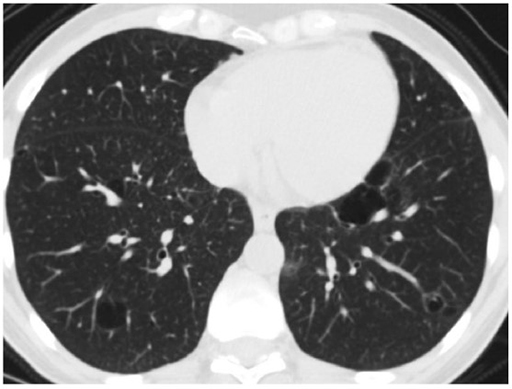
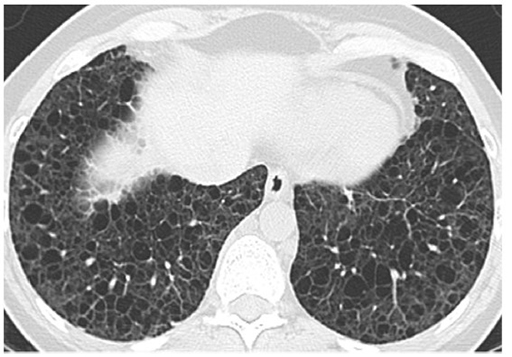
CXR and CT chest
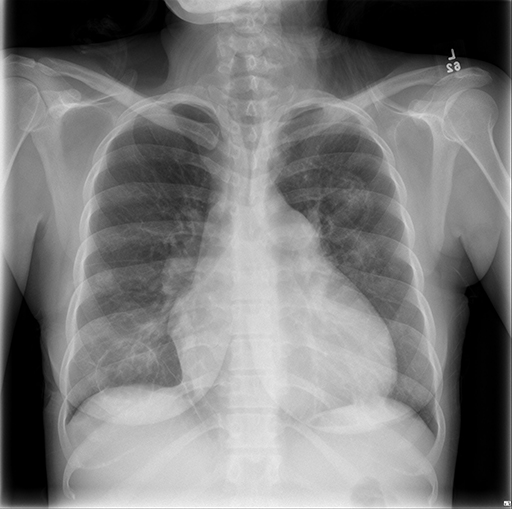
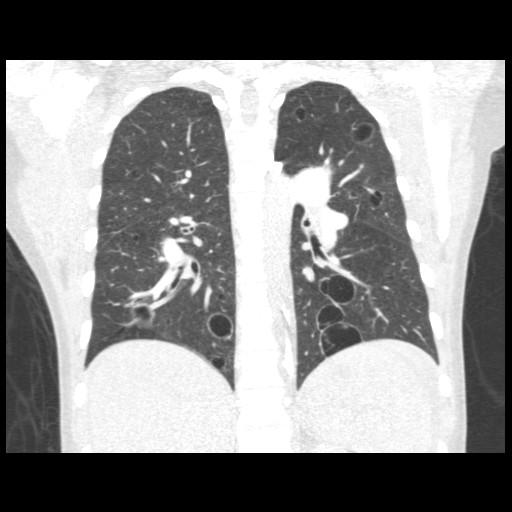
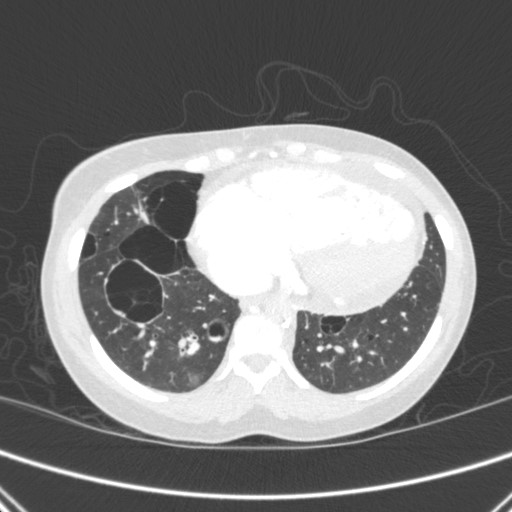
What is the most likely etiology of her diffuse cystic lung disease?
- Pulmonary Langerhans cell histiocytosis
- Lymphoid interstitial pneumonia
- Lymphangioleiomyomatosis
- Emphysema
Correct Answer 2
Work-up revealed HIV positivity. Subsequent pathology from transbronchial biopsies was consistent with a diagnosis of lymphoid interstitial pneumonia.
The Fleischner Society defines a cyst as a "round parenchymal lucency or low-attenuating area with a well-defined interface with normal lung and a wall thickness < 2mm." A cavity, on the other hand, has a wall thickness > 2 mm. Other cyst mimics include emphysema, pneumatoceles, bronchiectasis, and honeycombing.
Differential of Cystic Lung Disease
Pulmonary Langerhans cell histiocytosis
Lymphoid interstitial pneumonia
Lymphangioleiomyomatosis
Birt-Hogg-Dubé syndrome
Erdheim Chester disease
Follicular bronchitis
Sarcomas
Pleuropulmonary blastoma
Light chain deposition disease
Amyloidosis
Sjogren syndrome
Pneumocystis jiroveci
Recurrent respiratory papillomatosis
Desquamative interstitial pneumonia
Post-traumatic pseudocysts
We review the 3 answer choices here.
| Pulmonary Langerhans cell histiocytosis | Lymphoid interstitial pneumonia | Lymphangioleiomyomatosis |
|
|---|---|---|---|
| Clinical characteristics | 80-90% of patients are current or former smokers. Presents in young patients, M>F. | Commonly affects middle-aged women. Associated with connective tissue disorders and immunodeficiency states. | Young women. Can be sporadic or associated with tuberous sclerosis. Extrathoracic features include hepatic and renal angiomyolipomas and chylous ascites. |
| Presentation | About 2/3 present with cough or dyspnea. 15% present with a pneumothorax. | Cough or dyspnea | 40-50% present with a pneumothorax |
| Histology | Peribronchiolar infiltration by the Langerhans cells, leading to stellate nodule formation | Diffuse interstitial inflammatory infiltrate, usually around lymphatics | Smooth muscle cell infiltration of the lung parenchyma, airways, lymphatics, and blood vessels |
| Imaging |
Thick or thin-walled bizarre-shaped cysts in the upper lung that spare the costophrenic angles |
Cysts are usually few in number and distributed diffusely in both lungs or primarily in the lower lung
|
Diffuse thin-walled cysts that are round, ovoid, or polygonal
|
 |
 |
 |
References:
-
Gupta N, Vassallo R, Wikenheiser-Brokamp KA, et al. Diffuse cystic lung disease part I. Am J Respir Crit Care Med 2015;191(12):1354-1366.
-
Gupta N, Vassallo R, Wikenheiser-Brokamp KA, et al. Diffuse cystic lung disease part II. Am J Respir Crit Care Med 2015;192(1):17-29.
-
Hansell DM, Bankier AA, MacMahon H, et al. Fleischner Society: Glossary of terms for thoracic imaging. Radiology 2008;246:697-722.
-
Jawad H, Walker CM, Wu CC, et al. Cystic interstitial lung diseases: recognizing the common and uncommon entities. Curr Probl Diagn Radiol 2014;43:115-127.


