“Looking in the Mirror”
Matthew Gorgone, DO and Stephanie I. Maximous, MD, MS
Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Medicine, University of Pittsburgh Medical Center, Pittsburgh, PA
Case
A 56-year-old woman with a past medical history of hypertension and diabetes is three weeks into her hospital stay for COVID-19 pneumonia requiring , humidified high flow nasal canula. The pulmonary embolism response team is activated after she has a progressive increase in her oxygen requirement and the team performs point of care ultrasound (POCUS). The parasternal long axis and apical 4 chamber views that were obtained are shown below.

Question
What is the most likely diagnosis?
- Atrial septal defect causing right-to-left shunting
- Massive pulmonary embolism
- Pneumothorax
- Systolic heart failure
D. Systolic heart failure
Discussion
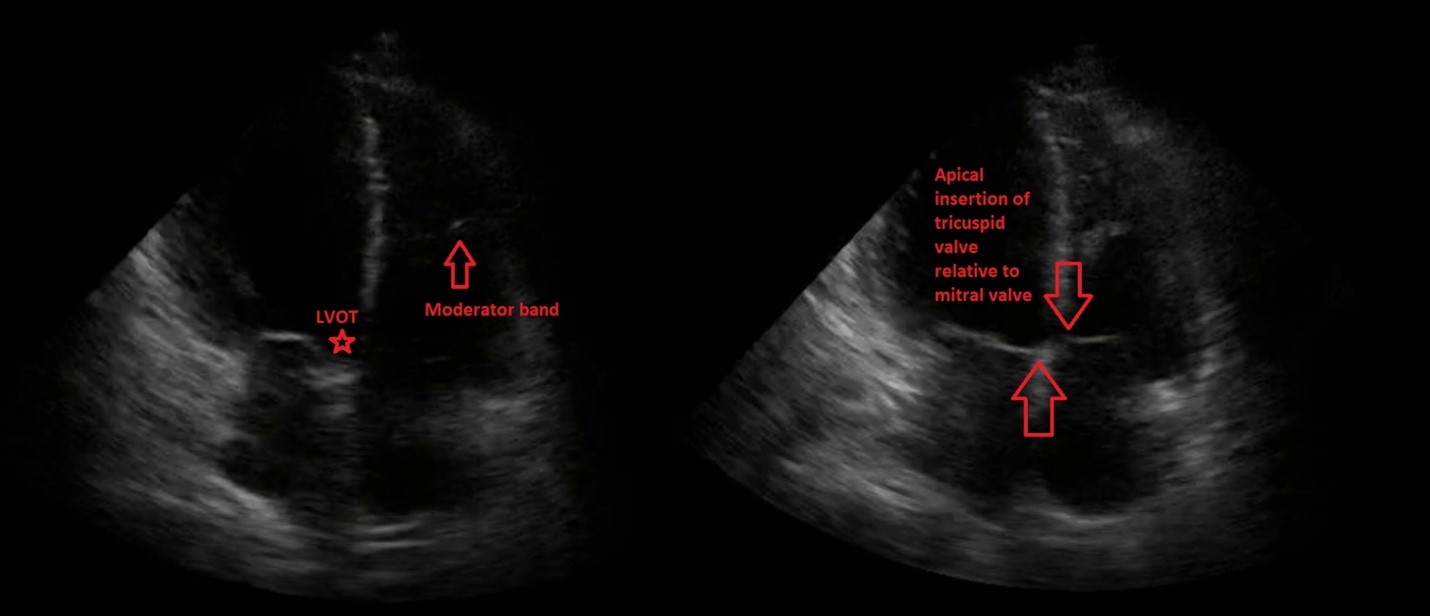
The images obtained show a parasternal long axis view with decreased left ventricular ejection fraction and a good quality, but ‘flipped’, apical 4-chamber view, with the probe marker in the 9 o’clock position rather than the 3 o’clock position. Note that the image would be considered the correct orientation at the Mayo Clinic. The ability to recognize the correct orientation is critical to avoid making false assumptions about ventricular size and function. There are several ways to differentiate left from right heart on apical 4-chamber view:
(1) The tricuspid valve is more apically displaced than the mitral valve.
(2) The right ventricle (RV) contains the moderator band which is a hyperechoic structure located near the apex of the RV.
(3) The left ventricular outflow tract is only present on the left side of the heart; this can be seen just medial to the mitral valve in the first portion of the clip.
There appears to be dropout of the intra-atrial septum which is more likely to be related to limitations in lateral resolution in the far field. Evidence of an atrial septal defect (ASD), from a transthoracic approach, would ideally be performed in the subcostal view aided by color Doppler. Right-to-left shunting across an atrial septal defect can be seen when patients are on positive pressure ventilation, when right atrial pressure exceeds left atrial pressure. This patient is not on positive pressure ventilation, making an ASD unlikely to be contributing to the patient’s hypoxia (answer choice A is incorrect).
In pneumothorax, exaggerated interventricular dependence (echocardiographic pulsus paradoxus) may be observed. There is no obvious septal shifting with respirations throughout the clip (answer choice C is incorrect). Systolic heart failure is more likely given the reduced ejection fraction seen on POCUS.
Massive pulmonary embolism is less likely to be causing the patient’s hypoxia because the right heart is not enlarged, and the right ventricular (RV) function appears normal based on gross visual assessment of the tricuspid annular plane systolic excursion (TAPSE) (answer choice B is incorrect). Although a normal appearing RV does not rule out pulmonary embolism, the more obvious abnormality is the reduced ejection fraction.
Echocardiographic findings in COVID-19 pneumonia include right ventricular dilation/dysfunction (39-47%), diastolic dysfunction (16-33%), and less commonly, systolic dysfunction (10-13%) with prevalence of all appearing to be more common in critical ill . 3,4 The right heart failure that is seen may be due to development of pulmonary hypertension in response to severe acute hypoxia as occurs in patients with ARDS, or due to concomitant submassive or massive pulmonary embolism.
This patient was diagnosed with systolic heart failure which, after negative ischemic workup, was suspected to be related to COVID-19. The patient received intravenous diuretics with improvement in her oxygen.
References
-
Oh JK, Kane GC, Seward JB, Tajik AJ. The Echo Manual. 4th edition. Wolters Kluwer; 2019
-
Ward RP, Lang RM. Pericardial Tamponade. Dynamic Echocardiography. Published online January 1, 2011:250-253. doi:10.1016/B978-1-4377-2262-8.00056-6
-
Szekely Y, Lichter Y, Taieb P, et al. Spectrum of Cardiac Manifestations in COVID-19: A Systematic Echocardiographic Study. Circulation. 2020;142(4):342-353. doi:10.1161/CIRCULATIONAHA.120.047971
-
Doyen D, Dupland P, Morand L, et al. Characteristics of Cardiac Injury in Critically Ill Patients With Coronavirus Disease 2019. Chest. 2021;159(5):1974-1985. doi:10.1016/j.chest.2020.10.056


