Pleural Effusion Confusion
Bryan Hay M.D, Department of Internal Medicine, University of Tennessee Health Science Center, Nashville
Case:
A 70-year-old female with a past medical history of asthma and hypothyroidism presented for evaluation of recurrent right sided pleural effusions for 3 months. She reported associated shortness of breath with exertion, dry cough, and an unintentional 20-pound weight loss over a period of 2 months. The patient underwent thoracentesis 3 times and pleural fluid analysis each time was consistent with an exudative effusion with mild leukocyte predominance. Pleural fluid flow cytometry, Acid Fast Bacilli (AFB), as well as bacterial and fungal cultures were negative. Her TSH was within normal limits. Due to recurrence of the effusion noted on CXR, a CT of chest, abdomen and pelvis was ordered (Figure 1 and Figure 2). Based on CT findings, she subsequently underwent hysterectomy and bilateral salpingo-oophorectomy. Biopsy of the bilateral ovarian masses showed ovarian fibroma.
Images:
Question:
What is the diagnosis?
- Ovarian hyper stimulation syndrome
- Meigs syndrome
- Pseudo - Meigs syndrome
- Luteinized thecoma
B. Meigs syndrome
Discussion:
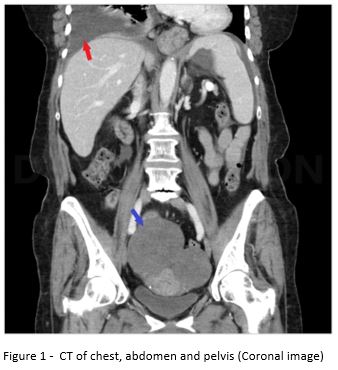
Figure 1 - CT chest, abdomen and pelvis (Coronal image) – Red arrow shows right sided pleural effusion and blue arrow shows bilateral ovarian masses. Minimal amount of intraperitoneal fluid also seen.
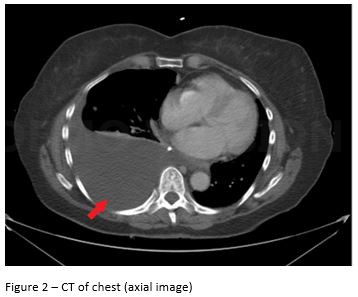
Figure 2 – CT of chest (axial image) – Red arrow re-demonstrates the large right sided pleural effusion in Figure 1
This patient was ultimately diagnosed with Meigs’ syndrome, which refers to the association of an ovarian fibroma or granulosa cell tumor with ascites and/or pleural effusion (1). In contrast, Pseudo-Meigs syndrome, refers to the association of ascites and/or pleural effusion with an ovarian tumor that is not a fibroma [choice C is incorrect]. Pseudo – Meigs could be due to a benign or malignant tumor . “Ovarian hyperstimulation syndrome occurs in the setting of an exaggerated ovarian response to fertility treatments resulting in ascites” [choice A is incorrect]. Luteinized thecoma is a benign tumor sometimes associated with sclerosing peritonitis causing large ascites [choice D is incorrect].
Given this patient’s advanced age, persistent symptoms and recurrence of her effusion, a CT scan of chest, abdomen and pelvis was ordered to rule out malignancy. Imaging showed a right sided pleural effusion, mild ascites and bilateral ovarian masses. Gynecological oncology was consulted. A CA 125 was ordered which was elevated up to 163 u/ml. She underwent hysterectomy and bilateral salpingo-oophorectomy. Histologic examination of the bilateral ovarian masses showed ovarian fibroma. Thus, the patient was diagnosed with Meigs’ syndrome. The patient’s clinical manifestations subsided after removal of the tumor and she remained asymptomatic during subsequent follow-up visits over the course of several months.
Meigs’ syndrome is a benign condition which can mimic an ovarian malignancy (2). The fluid accumulation is probably related to substances like vascular endothelial growth factor that increase capillary permeability (3). Removal of the tumor results in symptomatic relief in patients(1). There are many case reports that have described the association of Meigs’ syndrome with elevation of the tumor marker CA 125 (4). The patient mentioned in this case also had an elevated CA 125 despite the fact that her tumor was ultimately determined to be benign. Thus, in a post-menopausal female with a pelvic mass, the association of ascites, pleural effusion or elevated CA-125 may not always indicate an advanced ovarian cancer. Surgery and histopathologic examination are crucial because pathology aids in both diagnosis and treatment.
References
-
Meigs JV. Fibroma of the ovary with ascites and hydrothorax; Meigs' syndrome. Am J Obstet Gynecol. 1954;67(5):962-85.
-
Brun JL. Demons syndrome revisited: a review of the literature. Gynecol Oncol. 2007;105(3):796-800.
-
Ishiko O, Yoshida H, Sumi T, Hirai K, Ogita S. Vascular endothelial growth factor levels in pleural and peritoneal fluid in Meigs' syndrome. Eur J Obstet Gynecol Reprod Biol. 2001;98(1):129-30.
-
Timmerman D, Moerman P, Vergote I. Meigs' syndrome with elevated serum CA 125 levels: two case reports and review of the literature. Gynecol Oncol. 1995;59(3):405-8.


