The Pleura Doesn't Slide
Authors:
Sruti Brahmandam, MD
Bilal Athar Jalil, MD
Rodrigo Cavallazzi, MD
Division of Pulmonary, Critical Care and Sleep Disorders Medicine
550 S Jackson St, A3R40
University of Louisville
Louisville, KY 40202
Case
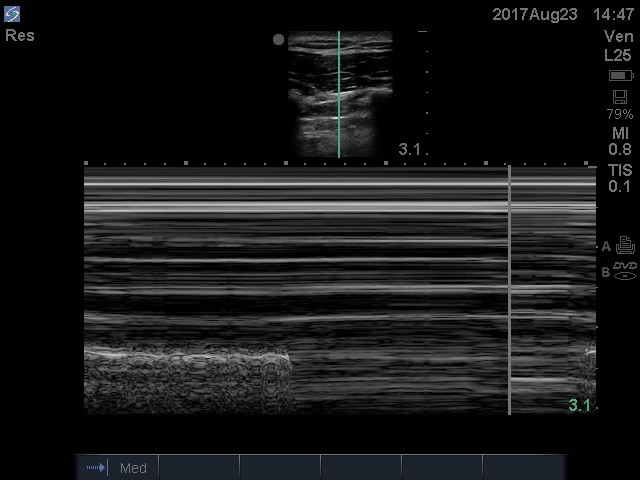
A 29-year-old female with history of intravenous drug abuse presented to the emergency department with sudden onset of chest pain and dyspnea. She was diaphoretic and appeared to be in moderate respiratory distress. Her heart rate was 120 beats per minute; her respiratory rate ranged in the mid-to-high 30s and was hypoxic requiring 4 liters of supplemental oxygen via nasal cannula. A point of care ultrasound performed in the emergency room of the left hemithorax is displayed as video 1 and the right hemithorax as video 2. The corresponding m-mode view of the right hemithorax is presented as image 1.
Images/Videos:
Image 1:
Video 1:
Video 2:
Question
What diagnosis is evident from the point of care ultrasound?
- Asymmetric pulmonary edema
- Right-sided pneumothorax
- Right-sided atelectasis
- Left-sided pneumothorax
- Left-sided atelectasis
B: ) Right-sided pneumothorax
Discussion
The ultrasound m-mode image is an example of a ‘lung point’ sign that is highly specific for diagnosing a pneumothorax (image 1). Lung sliding is seen as artifact created by the visceral-parietal pleural interface and is seen in the contralateral lung as displayed in video 1. The right lung is shown in video 2 and lung sliding is not seen because of the pneumothorax. This patient most likely developed a pneumothorax related to the rupture of septic pulmonary emboli from intravenous drug use. She underwent emergent chest tube insertion and decompression of the pleural space.
Point of care ultrasound is an extremely effective tool in patients with cardiopulmonary compromise. It provides a trained clinician quick answers by serving as an extension of the physical exam.1 The 2 commonly observed signs on lung ultrasound in the setting of a pneumothorax are the absence of lung sliding and the finding of a lung point. Although the absence of lung sliding has a lower specificity of 91.1% in the critically ill population2 and can be seen in other processes such as mucus plugging (causing severe atelectasis) or after pleurodesis, the finding of a lung point has a sensitivity of 66% and specificity of 100%.3 Overall lung ultrasound has a better diagnostic profile when compared to anteroposterior chest radiographs (sensitivity of 31.8% and specificity of 100%) and can be performed rapidly.4
To evaluate for a pneumothorax using ultrasound, the probe is placed on the anterior chest wall with the orientation marker pointing cephalad, and multiple intercostal spaces on both sides of the chest wall are scanned.5
Lung sliding is seen in a lung without a pneumothorax, but may not be appreciable in all patients. The use of m-mode makes this finding more apparent. A normal lung appears as a ‘seashore sign’ on m-mode while a pneumothorax will not show any lung sliding and will appear as a ‘barcode sign’. When both the barcode and seashore signs are seen on an m-mode image in succession as seen in image 1, it is termed a lung point, denoting the edge of the pneumothorax.
Though CT examination is the gold standard for diagnosing pneumothoraces, ultrasound can provide a diagnosis in a time sensitive manner in critically ill patients. 5 We highly recommend the use of lung ultrasound in addition to cardiac ultrasound in any cardiac arrest to evaluate for pneumothorax.
References
-
Wernecke K, Galanski M, Peters PE, Hansen J. Pneumothorax: Evaluation by ultrasound-preliminary results. J Thorac Imaging. 1987;2:76–8.
-
Lichtenstein, D A DA. "A Bedside Ultrasound Sign Ruling out Pneumothorax in the Critically Ill. Lung Sliding." Chest, vol. 108, no. 5, pp. 1345–8.
-
Lichtenstein D, Meziere G, Biderman P, Gepner A. The "lung point": An ultrasound sign specific to pneumothorax. Intensive Care Med. 2000;26:1434–40.
-
Nagarsheth, Khanjan K. "Ultrasound Detection of Pneumothorax Compared with Chest X-Ray and Computed Tomography Scan." American Surgeon, The, vol. 77, no. 4, pp. 480–4.
-
Husain LF, Hagopian L, Wayman D, Baker WE, Carmody KA. Sonographic diagnosis of pneumothorax. Journal of Emergencies, Trauma, and Shock. 2012;5(1):76-81.


