When You Can't Ease the Wheeze
Courtney Gushue, DO
Pediatric Pulmonary Fellow
Nationwide Children's Hospital
Columbus, OH
Case
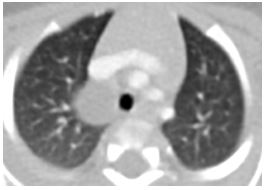
An 8-month-old, term infant with history of frequent vomiting is evaluated in the pulmonary clinic for persistent cough and wheeze. He has been tried on albuterol in the past without relief. He was previously on ranitidine for reflux concerns, but this has been discontinued as it did not make a difference clinically. Prior to this presentation, he had been treated for pneumonia once, and mom reports that he was "always sick" as a baby. Plain chest film was obtained and is shown below.
Image

Question
What is the abnormality demonstrated on the chest x-ray?
- Thymus
- Right sided aortic arch
- Congenital foregut cyst
- Shadow of overlying medical equipment
Answer: C) Congenital foregut cyst
Discussion
As part of the work up, a CT of the chest demonstrated a right sided, para-tracheal mass as noted in the image below. The mass was removed; pathologic examination was consistent with a benign congenital foregut cyst.
A foregut cyst is a closed sac lined with epithelial cells that develops abnormally during gestation, typically in the chest. It can originate from either the primitive gastrointestinal tract or the developing respiratory tract. It develops around the fourth week of gestation, when the ventral diverticulum from the foregut differentiates into a tracheal bud and subsequently branches to form the tracheobronchial tree. A bronchogenic cyst includes cilia and cartilaginous tissue that is found in normally developed airways and can be filled with mucus, fluid or air. This is in contrast to an enterogenic cyst, which is comprised of gastric and intestinal mucosa.
Bronchogenic cysts are the most common types of cysts found within the respiratory tract during infancy. 50% of them are located near the carina, but they can also be less often adjacent to the esophagus or alongside the trachea. Uncommonly, they are discovered within the parenchyma. They can be either symptomatic or found incidentally in adulthood when imaging is performed for another reason. When present, symptoms mirror those caused by other types of chest or mediastinal masses: wheezing, stridor or dysphagia from anatomic compression; cough; recurrent or post-obstructive pneumonia; hemoptysis; pleuritis; or rarely pneumothorax.
Suspicion for a foregut cyst may arise if a plain film of the chest demonstrates a mass with or without an air fluid level, when a CT scan shows a sharply demarcated cyst or when an MRI shows a cystic or solid lesion in the chest. They are often excised to relieve symptoms or to rule out other pathology. Complications of resection include air leak syndromes, rupture of cyst leading to infection, and nerve damage. After surgical excision, cyst recurrence has been documented, so caretakers should remain vigilant in the event of symptom recurrence.
References
-
Patel SR, Meeker DP, Biscotti CV, et al. Presentation and Management of Bronchogenic Cysts in the Adult. Chest 1994; 106(1): 79 – 85.
-
Abushahin A, Zarroug A, Wagdi M, et al. Bronchogenic Cyst as an Unusual Cause of a Persistent Cough and Wheeze in Children: A Case Report and Literature Review. Case Reports in Pediatrics 2018; https://doi.org/10.1155/2018/9590829.
-
Kendig's Disorders of the Respiratory Tract in Children. Seventh edition. Edited by Victor Chernick, Thomas F. Boat, Robert W. Wilmott, and Andrew Bush. 1111 pp., illustrated. Philadelphia, Saunders, 2006.


